


























News
Hitman, healer at centre of State’s murder case against Mashumi
MBABANE – A suspected hitman and a traditional healer are at the centre of the State’s case against Mashumi Andreas Shongwe. The two, according to the prosecutions provided crucial details...
Hitman, healer at centre of State’s murder case against Mashumi
MBABANE – A suspected hitman and a traditional healer are at the centre of the State’s case against Mashumi Andreas Shongwe. The two,...
IMF predicts slower growth
MBABANE – The International Monetary Fund (IMF) has projected that Eswatini’s economic growth will slow in 2026. This is reportedly because the country...
Luju showcase opens new growth paths for EU backed MSMEs
MBABANE – A showcase at the 2026 Standard Bank Luju Food & Lifestyle Festival has opened new commercial opportunities for livestock-based micro, small...
Entrepreneurs report positive results
MBABANE – A showcase at the 2026 Standard Bank Luju Food & Lifestyle Festival has opened new commercial opportunities for livestock-based micro, small...
SBS Bank goes live with eMACH.ai Treasury platform
MBABANE – SBS Bank Eswatini has taken another major step in its transformation into a full-fledged commercial bank. The new bank formed after...
Macadamia processing plant boosts Eswatini’s export ambitions
MATSAPHA – Eswatini’s rapidly expanding macadamia industry is poised for a major growth as Elangeni Food Group moves closer to commissioning its processing...
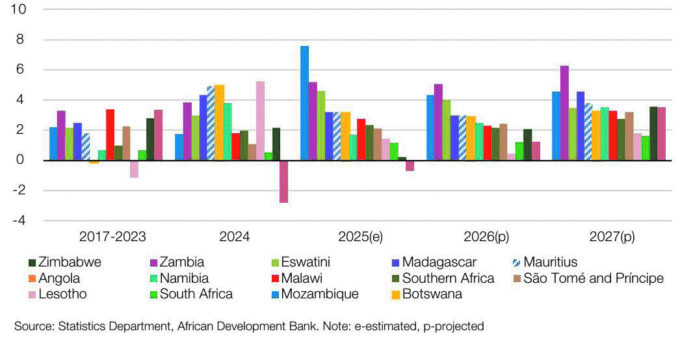
Eswatini among southern Africa’s fastest-growing economies
MBABANE – Eswatini is expected to remain among Southern Africa’s strongest-performing economies this year, with African Development Bank projections placing the kingdom third...

Inyatsi Construction building foundations of First World future
For more than four decades, Eswatini has witnessed one of the most significant periods of infrastructure development in its history. Under the leadership...
No more USA Visa processing in Eswatini
MBABANE – In a move that will significantly alter travel logistics for Eswatini nationals, the United States Embassy in Mbabane will cease accepting...
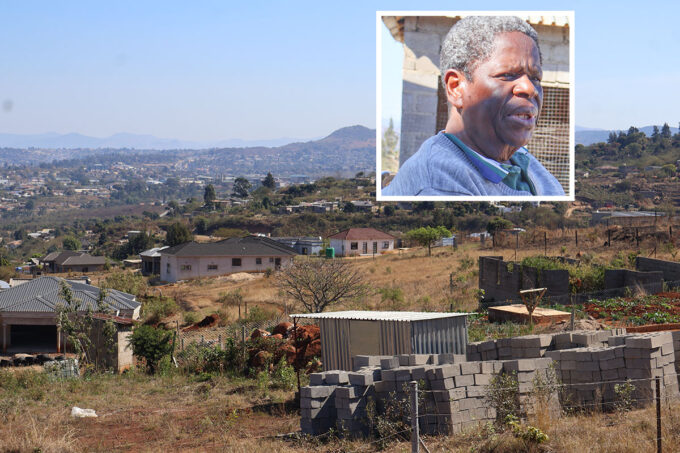
I don’t have money to compensate them – Polycarp
MONENI – Moneni overseer Prince Polycarp says he does not have the money to compensate the over 200 new homesteads that were settled...
King moves to save Ncangosini residents from eviction
KONTSHINGILA – Hundreds of residents living on a privately owned farm at Ncangosini, Kontshingila, are set to be spared from eviction after an...
Each MP set for E1m handshake
MBABANE – When the 12th Parliament assumed office in 2023, an ordinary Member of Parliament (MP) was earning a basic monthly salary of...
Latest Videos

Headlines 4 August
4 August 2026
REDEFINING INSURANCE INDUSTRY EXCELLENCE | LIDWALA MD | DR. THOKOZANI NKAMBULE
1 August 2026
HEADLINES | JULY 31
31 July 2026
HAEDLINES | JULY 29
29 July 2026
HEADLINES | JULY 28
28 July 2026
BIGGEST BRAAI 2026
27 July 2026
STORY BEHIND ESWATINI's ATHLETICS | THE FAST BREAK S1 E1
24 July 2026
HEADLINES | JULY 24
24 July 2026
How is Eswatini's Sugar Industry performing?
20 July 2026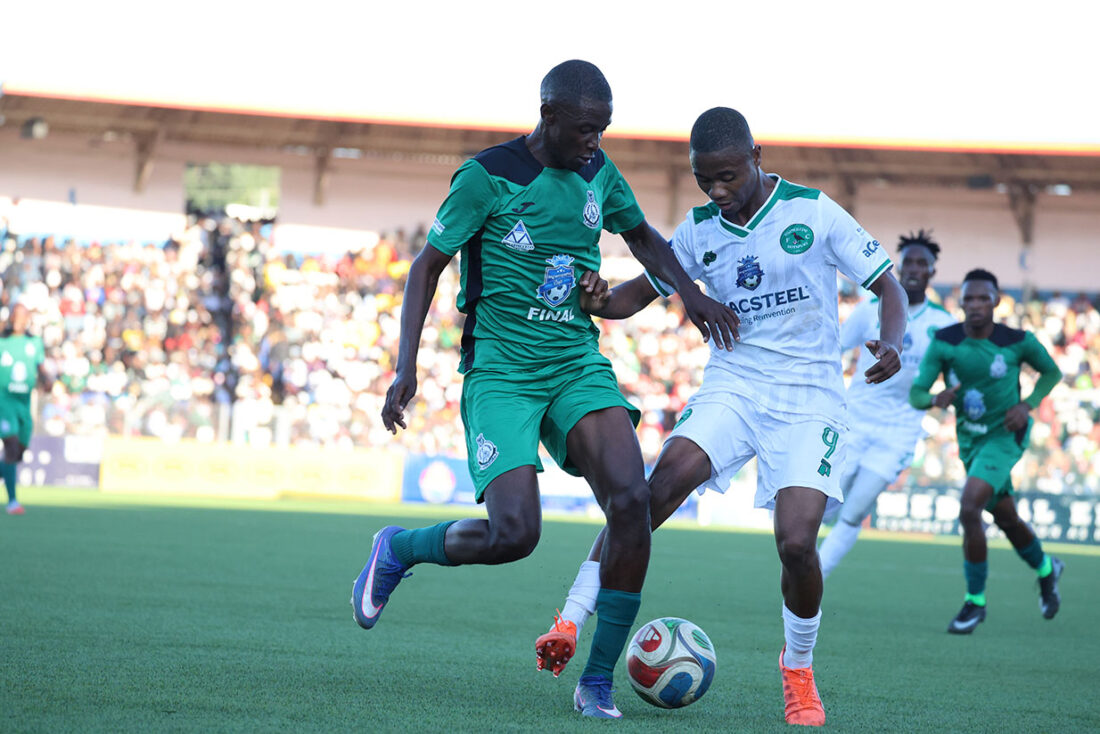
Sports
Kwakhe back to haunt Nsingizini!
MBABANE – Eswatini’s envoys in the upcoming CAF interclub competitions have discovered their opponents following a tricky preliminary round draw. The fixtures were officially revealed yesterday during the TotalEnergies CAF...





Comments and Analysis
Africa’s future demands less donor dependence
Africa’s youth have delivered a message many leaders have spent decades avoiding. While the abrupt withdrawal of USAID funding has revealed painful gaps...
Disaster is around too often
Venezuela and Japan. Then add to those the big hurricanes. The wildfires of France and Spain came out of the blue and into...

Economics of evictions: Displacement vs land acquisition costs
Thecountry constantly wakes up to issues of land tenure, which are more pronounced in farm evictions. This is a recurring issue that requires...

Parenthood, power: Challenging gender roles, expectations
Avideo triggered me recently, one about ‘sondlo’ as I mindlessly scrolled through my social media feeds ... then a thought hit me ......

Motoring
Jungle Rush FMX returnsto set Swazi Rally on fire
If you thought you've seen it all at the Swazi Rally, think again. The roar of engines is about to get even louder, the jumps even higher and the thrills...





Letters To The Editor
Is friendship still a blessing?
Madam, We live in a time where a majority believe in the cost and benefit theory. They do not stop at only believing in it, but they also go on...













{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}